This web page was produced as an assignment for Genetics 677, an undergraduate course at UW-Madison.
Like and Share this website!
What is Restless Leg Syndrome?
Restless Leg Syndrome, less commonly known as Willis-Ekbom disease, is a neurological disorder that is characterized by extremely unpleasant sensations in the lower legs (See Figure 1) that cause an irresistible urge to move [1,5]. The uncomfortable sensations typically worsen in the evening with inactivity and have been described as creepy-crawly, painful, burning, tingling, pulling, tight, twitching, and electrical current that can be temporarily relieved with constant movement. The discomfort of restless leg syndrome can also lead to sleep deprivation with difficulties falling asleep and staying asleep. In turn, these troubles with sleep can contribute to daytime drowsiness, troubles focusing, anxiety, depression, frustration, exhaustion, and an overall poorer quality of life [1-2]. It is estimated that restless leg syndrome is prevalent in 3-10% of the adult population in Western Europe and North America but has commonly been under diagnosed and misdiagnosed from poor understanding of the disorder. More diagnostic information is now becoming available and accurate diagnosis may result in a higher percentage of restless leg syndrome in the population. Late-age onset of primary restless leg syndrome is most common and usually develops between the ages of 40 and 60, although, early-age onset also occurs and is usually more severe [1]. Secondary restless leg syndrome is a result of another condition, such as iron deficiency, pregnancy, end stage renal disease, diabetes, rheumatoid arthritis, or spinal disorders, and may dissipate with control of the primary condition [1]. Studies have shown restless leg syndrome to be hereditary in 50% of cases and more common in women than men, a 2:1 ratio [2]. The increased risk in women may be based on secondary restless leg syndrome since women are more prone to iron deficiency with menstruation and pregnancy.
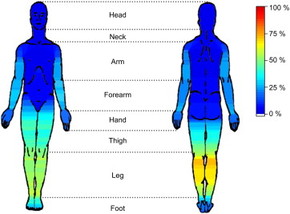
Figure 1: This image shows discomfort levels in restless leg syndrome patients, with yellow-red as the most severe discomfort and blue as the least. As depicted in the image, the most severe discomfort is in the lower legs, specifically the calf muscle [5].
Diagnosis and treatment
|
There are four clinical diagnostic criteria that must be met for restless leg syndrome: An urge to move the legs or other body parts usually accompanied or caused by unpleasant sensations, the urge to move or unpleasant sensations begin or worsen during rest or inactivity, the urge to move or unpleasant sensations are partially or totally relieved by movement, and the urge to move or unpleasant sensations are worse in the evening or at night or occur only in the evening or at night. It is essential that all four of these complaints be made in a diagnosis, if they are not, a mimic disease with similar symptoms may be responsible and should be treated appropriately [1]. There is no cure for restless leg syndrome but there are numerous ways to treat the symptoms. Before any treatment is administered, it is important to determine whether the patient has primary or secondary restless leg syndrome. Laboratory tests for renal and thyroid function, pregnancy, diabetes, and iron status (especially a serum ferritin analysis) are all possible and important tests to rule out cases of secondary restless leg syndrome. If there is no reason to believe it is secondary restless leg syndrome, primary restless leg syndrome may be diagnosed. A family history of restless leg syndrome or periodic limb movements are also suggestive of primary restless leg syndrome and can help lead with the diagnosis [2]. Some people with severe primary restless leg syndrome may also experience daytime restlessness [1].
There are multiple treatment options for severe restless leg syndrome, as Figure 2 displays [1]. If a patient has secondary restless leg syndrome, the primary cause should be treated. For example, if the patient is iron deficient, iron supplements (or a more iron rich diet) should be implemented and has been a very successful treatment. If a patient has low dopamine levels, dopamine agonists may be prescribed which help to increase the amount of dopamine your body produces. Benzodiazapines may be taken to help patients sleep through the symptoms. Alpha2 agonists help decrease involuntary muscle movements, like the uncomfortable sensations associated with restless leg syndrome. Anticonvulsants and opiates may be prescribed to help with really severe pain, although opiates are a last option as they can be very addictive [2,8]. For non-medicinal relief of symptoms it is recommended to avoid alcohol, caffeine, and nicotine, as these make you more restless to begin with, and to exercise, stretch, and massage your legs, especially before bedtime when the symptoms worsen [8]. |
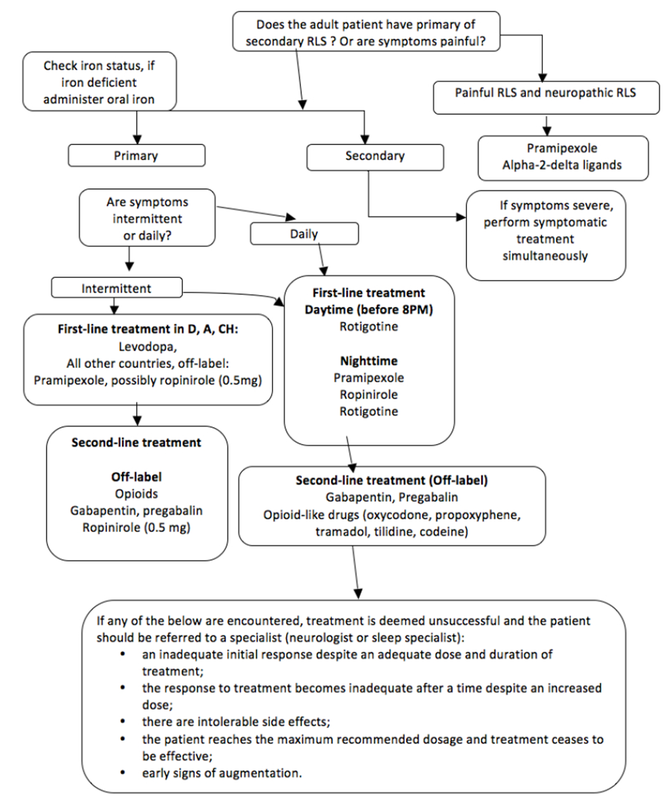
Figure 2: A treatment algorithm that may help clinicians determine the right method of treatment based on a patients symptoms [1]. Click on the image for a larger picture.
|
BTBD9

Figure 3: Location of the BTBD9 gene on the short arm of chromosome 6 is indicated at position 21.2 by the vertical red line [6].
BTB (POZ) domain containing 9, BTBD9, is a gene that has been associated with restless leg syndrome in two genome wide association studies. As of yet, little information is known about the function of BTBD9 in restless leg syndrome, but studies have confirmed a strong correlation with at least five single nucleotide polymorphisms in the DNA [3-4]. BTBD9 is located on the short arm of human chromosome 6 at the position indicated by the red line in Figure 3 [6]. This gene encodes the BTB (POZ) domain containing 9 protein (BTBD9 protein) which is involved in protein binding interactions and cell adhesion [12]. This protein has been moderately expressed in all tissues (See Figure 4), especially the brain and nervous system as BTBD9 is a neurological disorder [7]. Figure 4 shows the highest amount protein expression in the brain followed by moderate amounts in the thyroid, testis, ovary, lung, leukocytes, and heart [10] . BTBD9 protein has four domains, shown if Figure 5, that have functions relating to transcriptional regulation, substrate orientation, protein binding, and protein ubiquitination [11].


References
[1] Garcia-Borreguero et al. (2011). Algorithms for the diagnosis and treatment of restless legs syndrome in primary care. BMC Neurology
2011, 11:28. doi:10.1186/1471-2377-11-28
[2] Trenkwalder, C., Hogl, B., Winkelmann, J. (2009). Recent advances in the diagnosis, genetics, and treatment of restless leg syndrome. Journal of Neurology, 256: 539-553. doi: 10.1007/s00415-009-0134-9
[3] DeAndrade, M.P., et al. (2012). Motor restlessness, sleep disturbances, thermal sensory alterations and elevated serum iron levels in Btbd9 mutant mice. Human Molecular Genetics, Vol. 21, No.18. :3984-3992. doi: 10.1093/hmg/dds221
[4] Yang, Qinbo, et al. (2011). Association studies of variants in MEIS1, BTBD9, MAP2K5/SKOR1 with restless leg syndrome in the US populations. Sleep Medicine 12, 800-804. doi:10.1016/j.sleep.2011.06.006
[5] Georges Karroum, E., Leu-Semenescu, S., Arnulf, I. (2012). Topography of the sensations in primary restless leg syndrome. Journal of the Neurological Sciences, 320:1, 26-31. doi: 10.1016/j.jns.2012.05.051
[6] http://www.genecards.org/cgi-bin/carddisp.pl?gene=BTBD9
[7] http://www.ebi.ac.uk/gxa/gene/ENSG00000183826?ef=organism_part
[8] http://www.webmd.com/sleep-disorders/restless-leg-syndrome-treatment
[9] http://www.biomedcentral.com/1471-2377/11/28
[10] http://www-test.ebi.ac.uk/gxa/experiments/E-MTAB-513;jsessionid=8511CDEC703226FCFC06821C2A784508?serializedFilterFactors=&queryFactor&heatmapMatrixSize=50&displayLevels=false&displayGeneDistribution=false&geneQuery=btbd9&exactMatch=true&_exactMatch=on&_queryFactorValues=1&specific=true&_specific=on&cutoff=0.5
[11] http://smart.embl-heidelberg.de/
[12] http://amigo.geneontology.org/cgi-bin/amigo/gp-assoc.cgi?gp=UniProtKB:Q96Q07&session_id=3022amigo1362771715
** Cover photos credit: SleepDisordersGuide.com, FitAnGo.com
2011, 11:28. doi:10.1186/1471-2377-11-28
[2] Trenkwalder, C., Hogl, B., Winkelmann, J. (2009). Recent advances in the diagnosis, genetics, and treatment of restless leg syndrome. Journal of Neurology, 256: 539-553. doi: 10.1007/s00415-009-0134-9
[3] DeAndrade, M.P., et al. (2012). Motor restlessness, sleep disturbances, thermal sensory alterations and elevated serum iron levels in Btbd9 mutant mice. Human Molecular Genetics, Vol. 21, No.18. :3984-3992. doi: 10.1093/hmg/dds221
[4] Yang, Qinbo, et al. (2011). Association studies of variants in MEIS1, BTBD9, MAP2K5/SKOR1 with restless leg syndrome in the US populations. Sleep Medicine 12, 800-804. doi:10.1016/j.sleep.2011.06.006
[5] Georges Karroum, E., Leu-Semenescu, S., Arnulf, I. (2012). Topography of the sensations in primary restless leg syndrome. Journal of the Neurological Sciences, 320:1, 26-31. doi: 10.1016/j.jns.2012.05.051
[6] http://www.genecards.org/cgi-bin/carddisp.pl?gene=BTBD9
[7] http://www.ebi.ac.uk/gxa/gene/ENSG00000183826?ef=organism_part
[8] http://www.webmd.com/sleep-disorders/restless-leg-syndrome-treatment
[9] http://www.biomedcentral.com/1471-2377/11/28
[10] http://www-test.ebi.ac.uk/gxa/experiments/E-MTAB-513;jsessionid=8511CDEC703226FCFC06821C2A784508?serializedFilterFactors=&queryFactor&heatmapMatrixSize=50&displayLevels=false&displayGeneDistribution=false&geneQuery=btbd9&exactMatch=true&_exactMatch=on&_queryFactorValues=1&specific=true&_specific=on&cutoff=0.5
[11] http://smart.embl-heidelberg.de/
[12] http://amigo.geneontology.org/cgi-bin/amigo/gp-assoc.cgi?gp=UniProtKB:Q96Q07&session_id=3022amigo1362771715
** Cover photos credit: SleepDisordersGuide.com, FitAnGo.com
Site created by: Tara Pulvermacher
Contact e-mail: [email protected]
Last updated: 5/19/13
University of Wisconsin-Madison
Contact e-mail: [email protected]
Last updated: 5/19/13
University of Wisconsin-Madison
